NB: We advise you to print or archive this page, and to read the recommendations at the end.
Dear patient, we have just placed an implant-supported crown or bridge using CAD/CAM. This technique has many advantages, in particular
- There is no sealing cement which would melt under the gum and which is responsible for a very large number of failures in implantology,
- Your prosthesis is removable, so if there is any problem in the future we can remove it very easily.
It is important that you understand the construction of this type of prosthesis.
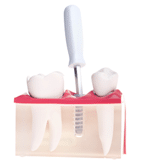
- Firstly, there is the titanium implant which is osseointegrated with the bone (welded into the jaw);
- Then the ceramic crown is bonded on an abutment that we call a Ti-Base (also made of titanium), a very specific part reserved exclusively for CAD/CAM;
- The whole thing is fixed, screwed onto the implant with a prosthesis screw (still in titanium);
- Then the screw head is protected with 2-3 well-compacted cotton pellets, and the screw hole is sealed with a light-curing composite.

This type of reconstruction is very reliable over time, however, as with any screwed or glued prosthesis, several things can happen:
- Over time, the composite block may wear out or even come off. Do not hesitate to consult quickly in this case so that the inside of the crown is not damaged. Any dentist can put back new cotton pellets and redo this type of composite.
- Then the screw that holds the crown to the implant may loosen. In this case you will feel something move slightly, or turn. It is important not to delay consulting a doctor, because screwing a crown back in is a benign act, but staying a long time with an unscrewed crown can lead to a fracture of the screw, which is much more annoying!
Any implantologist can screw a crown back onto an implant, but ideally a new screw should be used.
As we use different types of Ti-Base depending on the case, here is a list of the abutments used and the screws that go with them (feel free to contact us, and/or check your implant passport):
- MIS® brand Ti-bases (DENTSPY-SIRONA), MIS prosthetic parts with Internal Hexagon, which are screwed in at 30 NCm, the screwdriver used is a hex screwdriver of Ø 0.05′ - 1.27 mm (ML-LM005 for example). Ideally, a new screw should be used (ref: MN-S0160 for Narrow implant Ø 3.3 mm and MD-S0220 for the others). https://misimplants.fr/
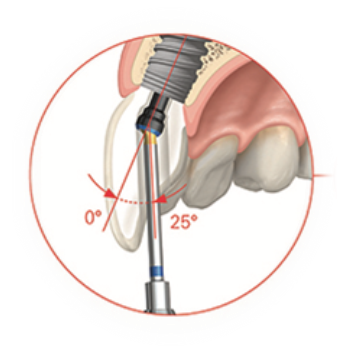
- Special case for the abutments with axis adjustment, called Ez-Base at MIS®. They are screwed at 25 NCm and require a Torx® type screwdriver (MT-ESM10). Ideally, a new screw should be used (ref: MN-E0160 for Narrow implant Ø 3.3 mm and MD-E0220 for the others. Check your implant passport). ATTENTION, because of the axis adjustment, it is not always possible to remove the screw from the prosthesis.
- C-Base® Ti-bases compatible with Zimmer® Tapered Screw-Vent from DESS®, screwed at 30 NCm and requiring a 0.05' - 1.27 mm hex screwdriver. Screw reference: SKU ZISV-018. www.dessdental.com

- Special case for abutments with axis adjustment, called Aurum Base at DESS®, screwed at 30 NCm and which require a Torx® Ball 06 type screwdriver (DT24TB06). The ideal would be to use a new screw (Torx® screw for AURUMBase® compatible with MIS® Seven or M4: SKU MISE-002). CAUTION, because of the axis adjustment, it is not always possible to remove the screw from the prosthesis. www.dessdental.com/fr-fr/mis
- Ti-Bases CEREC / inLab (DENTSPY-SIRONA), references Z TSV 3.5 and Z TSV 4.5 L, are screwed at 30 NCm, the screwdriver used is a classic hexagonal screwdriver of Ø 0.05′ - 1.27 mm. Screw reference: 6460575. CAUTION: no internal threads on these abutments (so no possibility of using an abutment puller).
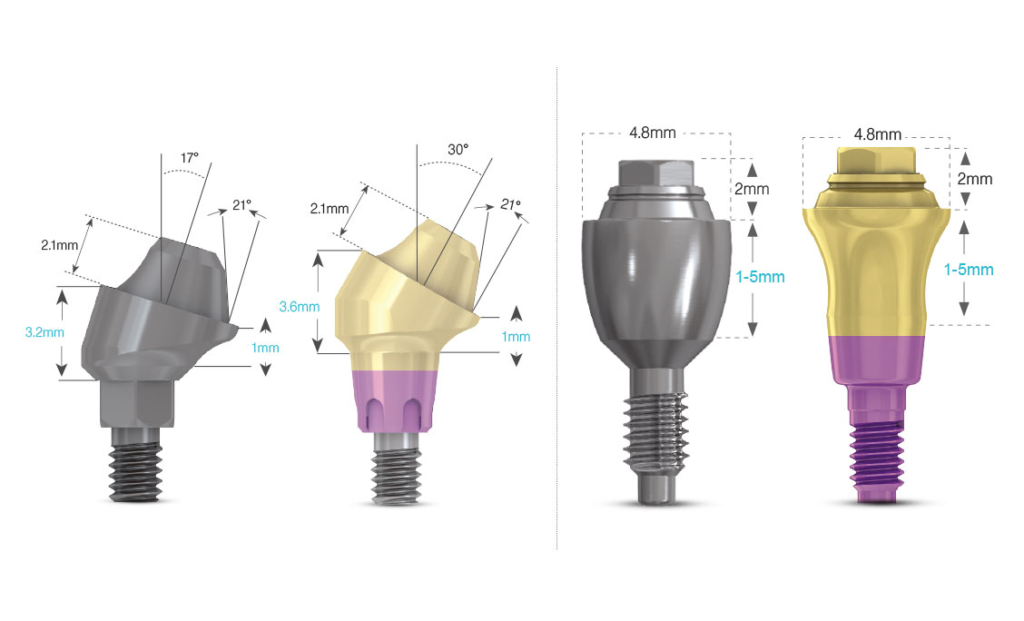
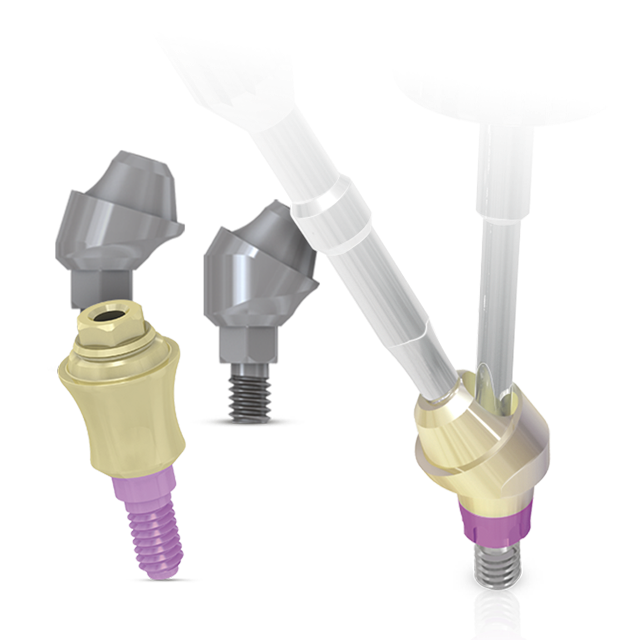
- For multiple-unit prostheses on MUA (Multi-Unit Abutment), All-On-X type or large bridges.https://misimplants.fr/
- The straight abutments are screwed in at 30 Ncm with the special screwdrivers MT-MURL2 or MT-MUML2.
- ATTENTION: Angled abutments are screwed in at 20 Ncm with the specific screwdrivers MT-MUL02 or MT-MMK07.
- The titanium prosthesis screws (MU-S0220) are screwed into the MUA abutments at 25 Ncm, with the conventional, hexagonal screwdriver Ø 0.05′ - 1.27 mm.

- Finally, the pillar is glued to the crown, these two elements can come off. In the same way, if you feel something moving, even slightly, you must consult quickly to avoid wearing out the parts. Not all implantologists are equipped to perform this type of bonding. Do not hesitate to contact us.
Finally, some important recommendations for the maintenance of your implant-supported crowns:
- First of all, we recommend that you use an electric toothbrush twice a day. Indeed, brushing crowns on implants is more complicated than brushing natural teeth, because the gumline is different. Electric toothbrushes are much more effective, especially on implants.
- The passage of interdental brushes on both sides of the implant is essential for the good maintenance of the implant. This should be done after brushing at least once a day and preferably in the evening. In the case of implants, the interdental space is often larger than in natural teeth, and conical brushes are often the best adapted to these spaces. If no brush is used, the risk of peri-implantitis is greatly increased. Peri-implantitis can lead to the loss of the implant.
- Flossing specifically for implants can also be very useful and effective in addition to brushes; especially for cleaning bridge pontics (this is the only method for cleaning under the pontic). We particularly recommend :
- GUM® ACCESS FLOSS
- or TePe® Bridge & Implant floss
- Be careful, if you wrap the wire around the implants as shown in the video above, you must do it very gently without forcing, so as not to damage the gum. We recommend that you pass it on both sides, and especially under the pontics.
- We recommend that you do not use a dental jet or hydropulper on implants. Indeed, these jets do not remove the dental plaque, so they give the illusion of cleanliness. But above all, the gum around the implants is much more fragile than around a natural tooth, and the pressure of the jet can "break" the gum attachment of the implant and propel bacteria under the gum... and thus create a peri-implantitis!
Thank you for your confidence

Our practice is equipped with an operating theatre, the nerve centre of our practice, which allows us to carry out all surgical procedures in optimal conditions of comfort and asepsis.
This is accessible via two airlocks: one for the patient and one for the nursing staff. This arrangement makes it possible to control hygiene and drastically reduce any risk of nosocomial infections. Before entering the surgery room, you will wear overshoes, a cap and a single-use gown. The patient lock also offers you the possibility to relax after the operation, to receive quietly the post-operative recommendations given by Stéphanie, our Qualified Dental Assistant and Head of the Operating Theatre.

In order to improve hygiene and asepsis control in the operating theatre, an air treatment system incorporating a High Efficiency Particulate Air Filter (HEPA) was installed and integrated into the air conditioning system. This device is capable of filtering out the finest particles (diameter greater than or equal to 0.3 µm) and eliminating dust formation in the operating area.

To improve the precision of the gestures during the most delicate interventions, the block is also equipped with a Carl ZEISS® operating microscope which offers a magnification of 20 times. Indispensable for certain operations such as Apical MicrosurgeryIt is a real plus in the performance of Sinus Liftor during difficult extractions.
In addition, our block is equipped with a whole series of devices to improve the quality of care or asepsis, such as a vacuum pump for sterile suction from A to Z, successive filters for the quality of the water in the hand-washing unit in the practitioner's locker, a motorised bridge table to adapt to all patient morphologies, a shape memory surgery chair for patient comfort, the PIEZZOCHIRURGY for safety during bone augmentation, a specific ceiling light for surgical lighting with calibrated colourimetry for better contrast, baseboard risers for easy cleaning of the floors, fully removable operating theatre furniture for optimal cleaning, a touch screen that can be operated with a sterile stylus so that you do not have to use a mouse or keyboard during surgery, a pass-through for direct access to the operating theatre, a radiology tube to check the patient's condition, and an X-ray tube to check the patient's condition. sterilisationA touch screen that can be handled with a sterile pen so that you do not have to use a mouse or keyboard during the operation, a pass-through for direct access to the patient's table, an X-ray tube to check an implant for example during insertion, music in the patient's locker and the operating theatre for a relaxed atmosphere, etc...
Everything is thought out beforehand to simplify the procedures and to make you as comfortable as possible during the treatment.

For some bone augmentation procedures, strict hygiene and aseptic conditions are required, and an operating theatre is preferable.
The French National Authority for Health (HAS) published a summary in 2008 on these subjects ("conditions for performing oral implantology procedures: technical environment"): "Bone ridge expansion, techniques using osteotomes such as Summers osteotomies, sinus floor enhancement with the use of intraoral bone harvesting material or bone substitute material and bone autografts can be performed in specific or adapted operating rooms or in the operating theatre. "
This site and its contents are the property of the CABINET DU DOCTEUR MICHAËL LUMBROSO
79 Ter Rue DE LA PAROISSE 78000 VERSAILLES
Tel : 01.39.50.24.66
Siret : 504-709-908 00025
SELARL of dental surgeons
Capital: €20,000
The texts on this site may not be used without the prior written consent of the owner. Dr Michaël LUMBROSO's office reserves the right to prosecute any act of infringement of its intellectual property rights, including in the context of criminal proceedings.
The reproduction of all documents published on the site is only authorised for information purposes and exclusively for private use. Any other use of these reproductions and in particular the use for commercial purposes is expressly forbidden, except with the prior written agreement of Dr Michaël LUMBROSO's practice.
The medical and health information on this site was written by Dr Michaël Lumbroso, Doctor of Dental Surgery.
The information made available on the site is intended to support, not replace, the relationship between a patient and their practitioner.
The site aims to inform patients about dental care and to present the practice to the general public.
No medical or personal information is collected via the site. An audience tracking tool (Google Analytics) is installed in order to improve navigation on the site.
This site complies with French legal requirements, including those concerning medical or personal information.
The site is fully funded by the SELARL Cabinet du Docteur Michaël Lumbroso. Moreover, no advertising is allowed and displayed on this site.
Only information provided by the practice's patients is retained by the practice.
The data communicated by Internet users when sending an e-mail from the website are not kept by the firm.
Dr. Michaël LUMBROSO has contributed his skills and experience to the training of practitioners for Dental Hi Tec, but has no financial or other interest with Dental Hi Tec. Dr Claire GONNETAN and Dr Isabelle LUMBROSO declare that they have no interest in companies and establishments producing or exploiting health products or in consulting organisations working on these products.
Google Analytics
Google analytics is installed on this website: To consult the privacy policy regarding the use of Google Analytics, please visit this link: http: //www.google.com/intl/fr/policies/privacy/. You can decide whether or not to receive cookies on your computer: I accept or I object
Your safety is an absolute priority for our practice, and we do everything possible to guarantee it. We have set up a real sterilisation chain, the main stages of which are described below.
The Sterilisation Cycle
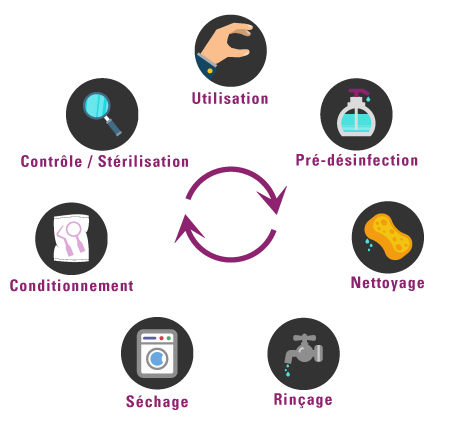
- PRE-DISINFECTION of instruments by soaking in a disinfectant solution in accordance with CE/NF standards.
- For some specific instruments: passage through an ultrasonic tank, which allows the removal of deposits.
- Installed in our thermodisinfector, it is a large washing machine that rises to over 93°C, and uses very powerful disinfecting agents.
It therefore cleans, rinses and dries the instruments in a cycle of about 1 hour. - PACKING of all instruments in sealed, single-use bags.
- Set up in one of our 3 autoclaves. These are steam ovens whose temperature rises to 135°C under 2 bars of pressure, which allows us to sterilise the instruments. Throughout this one-hour cycle, a computer integrated into the autoclave controls the progress of the operations. When the cycle is completed, and has been carried out in accordance with the standards in force, the computer authorises the printing of traceability labels.
- The TRACEABILITY labels are then stuck on each bag. These labels contain all the information concerning the cycle carried out (date and number of the cycle, identification of the autoclave, name of the person who controlled the operations, expiry date of the bag, etc.)
- At the same time, all the cycle parameters are stored in the cloud (temperature rise, pressure rise, duration, etc.).
- The instruments are then used during the care, and at the end of each procedure, the labels of all the bags used are scanned (there is a bar code) and entered in the patient file.
The various stages of the sterilization cycle (pre-disinfection, cleaning, rinsing, drying, packaging, control) are carried out and controlled by our qualified dental assistants: Stéphanie MAILLET, Céline SIERRA & Olesya SABOT (title registered in the Répertoire National des Certifications Professionnelles classified level IV, code CNIS 331S (decree of 02/10/2006 - JO of 24/10/2006).
Our autoclaves regularly undergo a series of tests to check the efficiency of the device. All of these tests are stored on the manufacturer's Cloud, containing all the information on the autoclave, as well as its qualification certificate from APAVE.




Some interventions may be contraindicated in certain situations.
Absolute contraindications
It is absolutely not possible to perform these procedures (such as implants, sinus lift, apical microsurgery, etc.) in the following situations:
- HEART: heart diseases affecting the valves (valvulopathies), recent heart attack, severe heart failure, cardiomyopathies.
- MISCELLANEOUS: certain bone diseases, cancer in progress, certain immunological diseases, immuno-suppressive treatments, AIDS declared, organ transplants pending, certain psychiatric diseases, highly irradiated jawbones (radiotherapy treatment), treatment of osteoporosis or certain cancers with biphospnonates.
Complications (in case of oral surgery or implants) CAN BE SERIOUS.
For children, it is not possible to place an implant before the end of the growth of the jaws (usually 17-18 years).
Relative contraindications
These interventions (such as implants, sinus lift, apical microsurgery, etc.) should be carried out with the greatest caution in the following cases: diabetes (especially insulin-dependent), angina pectoris (angina), seropositivity (absolute contraindication for declared AIDS), heavy smoking, certain psychiatric illnesses, cervicofacial radiotherapy (depending on the area, quantity of radiation, location of the cancerous lesion, etc.), certain autoimmune illnesses, drug and alcohol addiction, pregnancy. Specifically for the "sinus lift", the practitioner will act with caution in the following cases: sinus pathologies (chronic or acute sinusitis, polyps, aspergilosis, etc.).
Relative local contraindications
These operations (such as implants, sinus lift, apical microsurgery, etc.) should be done on a case by case basis, with caution in the following cases Insufficient bone, Certain diseases of the mucous membrane of the mouth, Periodontal diseases (loosening), gums must be cleaned and the disease stabilised beforehand, Severe bruxism (patient clenching his teeth), unbalanced occlusion ratio (between the upper and lower teeth), Infections in the neighbouring teeth (pockets, cysts, granulomas), important sinusitis, poor hygiene of the mouth and teeth.

This list is by no means exhaustive and contraindications are left to the discretion of the practitioner who examined you.
Immediate complications of implants
Anaesthetic risk, non-osteo-integration of the implant, infections, haemorrhages (not serious in most cases), nerve damage.
Late complications of implants
Late failure - several years after placement - may be due to mechanical factors, loosening of the implant (as with a natural tooth), lack of hygiene or poor general condition.
Contra-indications bleaching
Bleaching is not recommended in many cases, especially for children's and teenagers' teeth, as well as for teeth with caries, wear or abrasion lesions, hypersensitivity (teeth that are very sensitive to cold), large or non-tight fillings.
Bleaching products, especially if used in high concentrations or repeatedly, have a demineralising effect on the hard tissues of the tooth and increase their permeability; in addition to the risk of mechanical embrittlement of the tooth, the dental pulp may be more exposed to chemical and thermal aggression. Finally, these products react with dental filling materials (amalgams, composites) and can damage the junction between the tooth and the filling, thus encouraging infiltration and recurrence of caries.
In view of these risks and contraindications, an examination of the teeth and the oral mucosa by the practitioner is essential before any tooth whitening treatment.
Source : http://www.sante.gouv.fr/quels-sont-les-risques-y-a-t-il-des-contre-indications.html
Contraindications veneers
Contraindications are parafunctions (bruxism), occlusal disturbances (too much malpositioning of the teeth), teeth that are too decayed, or periodontal problems (gum disease).
In 1998, Michaël LUMBROSO finished his studies in Dental Surgery at the Paris VII faculty. He quickly joined his father, Dr Georges LUMBROSO, in the practice founded in 1974.
In March 2000, Michaël LUMBROSO defended his doctoral thesis in Dental Surgery (1), with a very honourable mention, congratulations of the jury, and the right to publish. This allowed an international publication (2).

Very quickly, he became aware of the importance of the well-being of patients during dental care, and was one of the first dentists to equip and train himself in painless anaesthesia, with the QuickSlepper® from DentalHiTec. Driven by the desire to transmit, he became a demonstrator and trainer for this company.
Doctor Georges LUMBROSO being one of the very first periodontologists and implantologists in the Yvelines, it is quite natural that Doctor Michaël LUMBROSO follows this path.
In 2005, he acquired a Carl Zeiss® operating microscope, and went to Philadelphia, University of Pennsylvania to further his training in microsurgery (3).
Dr Michaël LUMBROSO continues his training in implant and periodontal surgery by obtaining in 2009 a Post Graduate in Implantology & Periodontics (Penn-University Philadelphia, USA), and in 2010 a University Diploma in Maxillofacial Surgical Rehabilitation (Hôpital Saint-Louis, Paris VII), a diploma recognised by the French National Order of Dental Surgeons.
This diploma allows him to direct his professional practice towards implantology, and particularly pre-implant bone augmentations such as Sinus Lift.
In 2011, he followed a thorough training in Implant Surgery at the IFCIA (Institut de Formation en Chirurgie Implantaire Avancée). This training allows him to propose the "All-on-4, or All-on-6" techniques in the implant treatment of complete dentures This training allows him to propose the "All-on-4" or "All-on-6" techniques in the implant treatment of: reconstructing a complete arch (12 teeth) with only 4 or 6 implants; and the techniques of Immediate Esthetic Treatment.
At the same time, he created in March 2010, the dental practice "Dental Harmony", based on theGlobal Approach, Prevention and Well-being, in order to help patients to find a dental harmony.
This 170m2 technical platform allows the integration of all the equipment necessary for 21st century dentistry (operating theatre, operating microscope, dental panoramic, Cone Beam, complete CAD/CAM chainetc.).
In 2012 he is the founder and president of the Association Dentiste en France. The aim of this association is to defend French dentistry based on a Quality approach, on the well-being of our patients, on the development of Prevention and Prophylaxis, because today we know how to "treat our patients before they get sick!
It is in this context that Dr Michaël LUMBROSO participates in several TV programmes on the Yvelines Première channel(see videos), writes articles in the professional press, and gives conferences for the Efficience Dentaire company, for example, and participates in round tables on prevention.
In 2014, he was a speaker at the 3rd Assises des Soins Coordonnés at the Conseil économique, social et environnemental on the theme: Periodontitis and Systemic Diseases.
In 2019, it decided to take the digital turn and acquired a complete CAD/CAM (Computer Aided Design and Manufacturing)chain: the CEREC®.
This chain makes it possible to take optical impressions with a camera, to merge bone scan files with these optical impressions, to produce surgical guides for even faster and more precise implantology, to produce ceramic dental crowns, inlays in one session, veneers, etc.
At the end of 2019, all the dental assistants and practitioners of the practice will receive advanced training in denture make-up by the Ivoclar® company.
Today, he devotes himself full time to his patients and to the development of Dental Harmony.
- Periodontal Manifestations of Congenital Systemic Diseases in Children " . Nominated to represent the Paris 7 Faculty, at the 2002 ADF/DENTSPLY Thesis Award, Alpha Omega Jacques Breillat Thesis Award.
- Interest of granulocyte growth factors in some early periodontitis of systemic origin. M. LUMBROSO, C. NAULIN-IFI, I. BAILLEUL- FORESTIER. Journal d'Odonto-Stomatologie Pédiatrique Vol.10-2, 49-56, 200.
- Training Course in Endodontic Microsurgery, University of Pennsylvania, USA under the supervision of SYNGCUK Kim, DDS, Ph.D.
What is tooth decay?
Few people know this, but tooth decay is an infectious disease.
According to theWHO*, it is probably the most widespread disease in the world, affecting 3 billion people. Depending on the country, it affects between 60% and 90% of the population. And yet it is a simple infection whose mechanisms have been known for a long time, and the bacteria clearly identified(mainlyStreptococcus Mutans and Lactobacillus Acidophilus ).
It is thought to have appeared during the Neolithic period (about 7000 years ago in Europe), probably in connection with the consumption of cereal flour. Prehistoric man was free of cavities. Caries is therefore not inevitable...
Sources: https://www.who.int/fr/news-room/fact-sheets/detail/oral-health
How do cavities form?
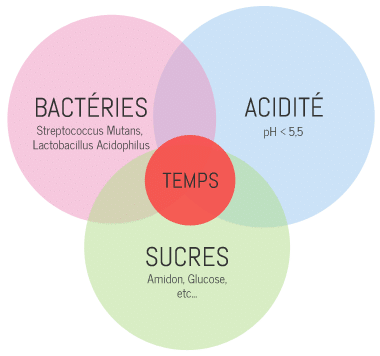
Caries is the consequence of a bacterial imbalance in the oral flora. For a cavity to form, 5 factors must come together.
- It requires the presence of certain so-called "cariogenic" bacteria such as Streptococcus Mutans and Lactobacillus Acidophilus. We all carry these bacteria (in greater or lesser quantities). These bacteria organise themselves and form dental plaque.
- Acidity is necessary, in fact below a pH of 5.5 the risk of caries is clearly increased. However, some foods are very acidic (Coca-Cola, for example, has a pH of 2.3), the degradation of food by certain salivary enzymes increases acidity, and finally, certain bacteria, such as Streptococcus Mutans, generate the acidity they need.
- Sugar (carbohydrates) is needed to feed the cariogenic bacteria. However, our "modern" diet is very rich in carbohydrates, and sticky ones at that.
- There are certain predispositions to tooth decay depending on the composition and resistance of the enamel, the quality and quantity of the saliva, etc. But what must be understood is that without bacteria there is no decay.
- In addition to the above four factors, it takes time. That is, the bacteria must be present long enough, in an acidic environment, and in the presence of sugar for them to begin to dissolve enamel.
When these five factors are combined, cariogenic bacteria multiply and the acids produced by these bacteria will dissolve the enamel. The bacteria then penetrate the tooth. The microbes can then enter the deepest layers of the tooth (the dentin, then the pulp), dissolve the dental tissue, and destroy the tooth from the inside.
Read Dr Lumbroso's interview on caries

What can be done to prevent cavities?
All five factors need to be addressed at the same time.
I - Brushing your teeth.
Tooth brushing is a decisive element in the fight against tooth decay, it will allow to disorganize the dental plaque, to decrease the bacterial mass, and especially it will play on the time factor. This is why you should brush your teeth at least twice a day, so that between two brushings, the bacteria do not have time to reorganise. It is preferable to brush your teeth after meals, in order to eliminate the bacteria and the food that has been deposited during the meal, and to reduce the acidity. In addition, some toothpastes polish the surface of the enamel, which slows down the re-attachment of bacteria to the tooth.
As you will have understood, brushing acts on all the factors of caries formation, it is the "keystone of prophylaxis ". We recommend the use of electric toothbrushes combining rotation and pulsation movements, the effectiveness of which has been scientifically proven. We pay particular attention to brushing, so all our patients receive a prescription adapted to their needs. In some cases, the toothbrush is not enough, it must be supplemented by dental floss or interdental brushes.
II - Food
The diet will influence important factors: acidity, sugars, and time. It is absolutely necessary to limit the intake of soft drinks, as they are (very) acidic and sweet. Even sugar-free soft drinks are cariogenic because of their pH. If you can't do without soft drinks, it is better to drink them through a straw, in order to reduce their contact with the dental surfaces, and then drink a little water...
Nibbling on sweets, biscuits (all cereal-based products are broken down into sugars when they come into contact with saliva), etc., encourages the development of cavities because it affects the three factors of sugar, acidity and time. When we say carbohydrate-rich foods, we immediately think of sugars and sweets. But carbohydrate-rich foods do not necessarily taste sweet. The starch in potatoes, but also in cereals and flours, is just a long chain of sugar that certainly does not taste sweet. When we eat salted biscuits, crisps and chips, these are carbohydrate-rich products. The softer and stickier a food is, the more cariogenic it is.
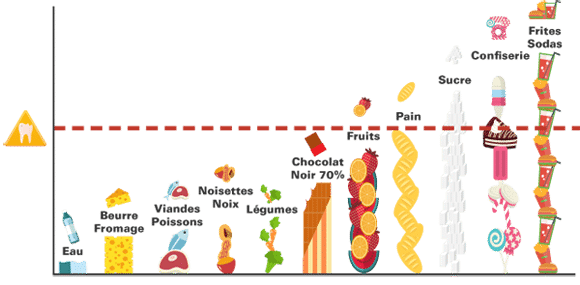
Foods can therefore be classified according to their cariogenic potential:
- At the bottom of the ladder, water.
- Dairy products and fats (cheeses are excellent protective foods to finish a meal).
- Meat and fish.
- Nuts, hazelnuts, peanuts rich in fat to be preferred to extruded products as an appetizer.
- Vegetables.
- Dark chocolate, rich in cocoa.
- Fruit: presence of fructose and acidity. Beware of the apple crunching as a substitute for brushing.
- Bread, flour, rice and potatoes are all more cariogenic when cooked.
- Sugar.
- Confectionery, sucrose, honey.
- Cereal bars, breakfast cereals.
- Snack biscuits, chips, soft drinks and colas, bananas, sultanas.
III - Fluorine
The consumption of fluoride during childhood allows this protective element to be integrated into the constitution of the enamel in formation. Fluorinated enamel is more resistant to caries. At a local level, fluoride plays an antibacterial role and protects against caries. This is why it is recommended to consume fluoridated table salt (if the tap water is not too fluoridated), and to use a fluoridated toothpaste.
IV - Chewing Gums
Chewing gum helps to fight tooth decay, but chewing gum will never replace a good brushing, but it can be beneficial when you cannot brush your teeth after a meal. Of course, only sugar-free chewing gum should be consumed. Why is chewing gum beneficial? First of all, chewing increases the flow of saliva, which dissolves sugars, and fights acidity. This is because saliva has a number of chemical agents that help to raise the pH. The stickiness of chewing gum helps to clean the teeth and remove food residues. In addition, certain sweeteners such as Xylitol contained in certain chewing gums have a bacteriostatic effect on certain cariogenic bacteria. Finally, some chewing gums contain fluoride. So let's chew.
V - Other
Certain diseases such as diabetes, certain treatments that reduce salivation, can favour the appearance of caries. We can help these patients thanks to a complete caries assessment (salivary tests, bacterial tests, etc.), and a global treatment.
A short explanation of dental implants
For many years, Dr Lumbroso's practice in Versailles (78) has been practicing dental implantology. As an expert, Dr. Lumbroso offers you some explanations:
Dental implants have been around for more than 30 years and are now the best solution for replacing missing teeth while preserving the remaining healthy teeth. Indeed, it allows to replace the missing tooth without any trauma of the adjacent teeth, contrary to the bridge (bridge between two teeth).
Only a precise diagnosis allows us to correctly evaluate the cost of the rehabilitation, due to the choice of the implant and the specific constraints of each patient.
Indeed, the practitioner adapts the length, diameter, shape and number of implants to the clinical case thanks to an X-ray examination: the 3D Cone Beam, a kind of mini scanner, available in our practice.
An implant is a kind of artificial root made of titanium, fixed in the bone like a natural tooth.
The implant protocol
First of all, the practitioner has to access the bone, he removes the gum in order to have a good view of his operating field. Today, 3D scanners reproducing the precise anatomy of the jawbone on a computer allow for a much less invasive surgery in common cases (the so-called "flapless" technique).
After the implants are placed, there is a healing period of two to three months. During this phase, a particular process will occur, it is the OSTÉOINTÉGRATION of the implant. Indeed, the bone tissue has the particularity of being able to "weld" to the titanium of the implant. At the end of this period, the implant is completely "one with" the jawbone, it only remains to take an impression to make the final prosthesis.
In some cases we can even place the implant on the day of the extraction, in order to minimize the number of interventions. In the case of anterior teeth, for obvious aesthetic reasons, we can make a temporary crown directly on the implant, the day it is placed. This is called Extraction - Immediate Implantation. Thus, in the same session, a condemned tooth can be replaced without the patient ever being toothless.
Implantology is an essential breakthrough that has improved the lives of thousands of patients. Indeed, it is often the optimal solution because :
- Implants are currently the most comfortable and reliable solution over time
- This avoids unnecessary "sacrifice" of healthy teeth
- This is the only way to avoid a removable prosthesis
- The patient regains the comfort of his original teeth and thus an incomparable quality of life
- The aesthetics are optimal
- This avoids bone loss following tooth extraction.
Simply put, a dental implant is the optimal solution if one or more teeth are missing. This means that almost everyone can have a replacement for their teeth, with the same appearance and function as a natural tooth. However, it is important to have fully developed bone tissue beforehand. For this reason, dental implants are not normally placed in people under the age of 18.




When and why use Apical Microsurgery?
We perform Apical Microsurgery when traditional practice does not allow us to reach a lesion located at the root tip.
When endodontic treatment and root canal filling are partially completed, infection may develop.
Thanks to the precision provided by the operating microscope, this operation allows a cure in a large proportion of the cases treated.
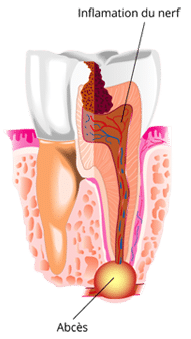
In the incompletely treated canal, the remaining pulp becomes mortified and bacteria proliferate in the unfilled portion of the canal.
A lesion(granuloma) forms at the end of the root, in the bone and ligament.
Untreated granuloma will most often progress to cyst andabscess.
The first step may be to repeat the root treatment (orthograde treatment).
When orthograde treatment does not allow the canal to be cleaned to its end, only Apical Microsurgery can remove residual bacteria.
How?
Apical resection is the surgical removal of the remaining cyst. The root tip is cut to sanitise the infected area. The bone cavity is carefully cleaned of all cystic debris.
The end of the canal is hermetically sealed, this is the retrograde obturation under the operating microscope. Only the use of a operating microscope (magnification x25) allows to work on such small surfaces.
Bone healing gradually fills the cavity left by the operation. After several months, the bone has healed and the infection has completely disappeared.
Benefits
We make precise and small incisions under a microscope. Our operations are therefore better controlled, without unnecessary damage, and the procedures performed are very precise. We thus respect the concept of "minimal surgery" and our results are all the more satisfactory.

When and why do we whiten our teeth?
Tooth whitening is used to lighten the colour of the teeth, the correct term is tooth lightening.
These techniques are reserved for special cases and should not be used as an excuse for poor oral hygiene.
The colour of the teeth is influenced by different elements:
- EXTRINSIC stains: outside the tooth = Nicotine, Coffee, Tea, etc. stains
- INTRINSIC stains: inside the tooth = natural stains, stains due to antibiotics taken during childhood, enamel anomalies etc...
Tooth whitening removes or reduces intrinsic discolouration by using a hydrogen peroxide derivative that penetrates the enamel to dissolve the pigments at the enamel/dentin junction.
Outpatient gutter treatment includes:
- A preliminary dental check-up, to see if a lightening is possible and recording of the initial shade.
- Taking impressions of the upper & lowerjaws.
- The production of the 2 thermoformed gutters for the product.
- The supply of the product(Carbamide Peroxide for bleaching, Amorphous Calcium Phosphate, to reduce sensitivities, and even to strengthen and remineralize the enamel) until the desired shade is obtained.
- Control visits to check the progress of the colour.
- Polishing if necessary.
These trays will be applied every night for about two weeks or for 2 hours a day. The patient inserts the whitening gel into the tray and wears it for a period of time determined by the practitioner. During the treatment, the teeth are a little more sensitive to temperature differences, which is why we recommend the parallel application of fluoride gels.
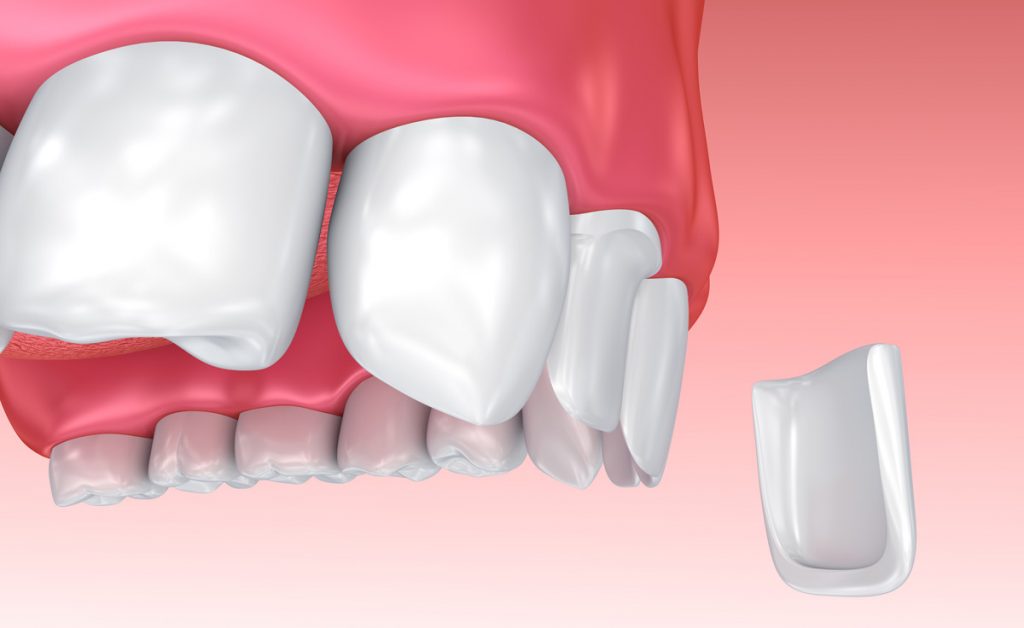
The Facets
Veneers are ceramic coatings that are bonded to the tooth. This new technique allows a clear improvement in the aesthetics of the smile.
Objectives:
- Correcting the colour of teeth when bleaching is not enough.
- Correcting tooth shape anomalies.
- To improve aesthetic problems related to slight malposition of the teeth.
The realisation :
Thanks to our CAD/CAM system, we can produce veneers in-house, sometimes in one day! Preparation, optical impression, design of the veneers on our software, machining of the parts, make-up, baking and fitting the same day. Changing your smile in one day is now possible.
Please note that this is not systematically the case, it is only possible for some facets in simple cases. Do not hesitate to ask us for more details.