History
Since the 1970s, dental implants have been a major advance in the replacement of lost teeth.
Thanks to a minimally invasive procedure, they allow the patient to smile again and chew efficiently. They are currently the most comfortable solution, and the most reliable over time (97% success rate in implantology). They avoid wearing a removable prosthesis (dental appliance) or the mutilation of healthy teeth to make a bridge (bridge between two teeth).
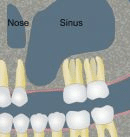
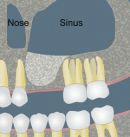
In fact, dental implants do have one constraint... In order to place an implant reliably, sufficient bone volume is required. In the upper jaw, above the molars, there is a hollow cavity in the middle of the jawbone, this "pneumatic cavity": it is the maxillary sinus. The maxillary sinus is lined with a mucous layer: this is Schneider's membrane. Very often, when the maxillary molars are extracted, the amount of residual bone under the maxillary sinus is too small to be able to place implants (at least 8 mm of bone is needed to place an implant). What can be done?
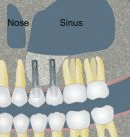
As early as the 1970s, practitioners had the idea of performing a bone augmentation under the maxillary sinus, by removing Schneider's membrane and interposing a filling material.
Today, there are two techniques for bone augmentation under the sinus:
- Elevation and partial filling of the maxillary sinus by the alveolar (or crestal) route, known as the Summers technique.
- Elevation and partial filling of the maxillary sinus using the Tatum technique or " Sinus Lift ".
These two techniques have different indications.
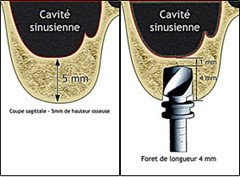
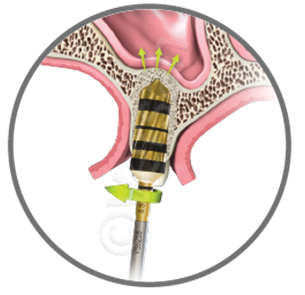
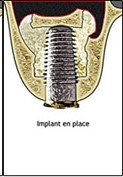
Summers' technique
The Summers technique can be used when at least 5 mm of bone remains beneath the sinus. It involves "pushing" the sinus membrane through the alveolus created for implant placement. This is now achieved by special drills that rotate in the opposite direction, which collect bone chips during drilling, condense them and gently inject them under the sinus membrane, which is then gently pushed. Depending on the volume of bone to be gained, a filling material can be interposed before the implant is placed, in the same operating time. The post-operative course is generally minor.
Sinus Lift
Le Sinus Lift est réservé aux pertes osseuses plus importantes (hauteur résiduelle < 4-5 mm). Il s’agit de réaliser une fenêtre osseuse en regard du sinus maxillaire, puis la membrane de Schneider est minutieusement décollée. Un matériau de comblement est ensuite glissé sous cette membrane, et la fenêtre est refermée. Il est parfois possible de placer les implants en même temps, mais dans la plupart des cas, il est préférable de laisser cicatriser 3-4 mois et de poser les implants après un contrôle radiographique 3D. Les suites postopératoires sont plus importantes qu’avec la technique de Summers, elles sont comparables à l’extraction de dents de sagesse incluses. Œdème et hématome surviennent parfois.
Benefits
These two meticulous operations require a large technical platform and an experienced team. This is why Dr Michaël LUMBROSO holds a University Diploma in Maxillofacial Rehabilitation Surgery(University of Paris VII), and is fully qualified to perform this type of operation. Indeed, the main risk of these operations is a tear of Schneider's membrane without the practitioner noticing it.
This is why in our practice these procedures are carried out in our operating theatre, under rigorous aseptic conditions(sterilisation chain, HEPA filter, traceability, etc...). During a Sinus Lift, in order to limit the risk of tearing the Schneider's membrane as much as possible, we use a very special instrument: the PIEZZOCHIRURGY. This instrument uses ultrasound and allows the bone window to be made without damaging the membrane underneath, as it is inactive on the soft tissue.
Moreover, in our practice, this procedure is performed under an operating microscope. This considerably increases the precision of our actions, and thus reduces the risk of tearing the membrane. And if a perforation should occur, it is almost impossible for it to go unnoticed thanks to the operating microscope. The operation is then stopped and the window closed, without any consequences for the patient's health. However, it will be necessary to intervene again after a few weeks.
What is a Zirconia crown?
A zirconia crown is a laminated ceramic crown, it consists of two distinct layers:
- A zirconium oxide cap, made by CAD/CAM(Computer Aided Design and Manufacturing).
- A surface part called "cosmetic" made of traditional ceramics mounted and fired layer by layer by a traditional ceramist.
- Not to be confused with a "Full Zirconia" crown, which consists of a single monolithic block of zirconia which is then made up.
The zirconia crown is nowadays the Nec Plus Ultra The zirconium crown is the most popular choice for dental crowns, especially in difficult anterior cases and/or when metal needs to be concealed, for example.
How is the zirconia coping made?
- A traditional impression of the tooth is made by your dentist.
- or even better, we can make a digital impression directly with the optical camera of our Digital CAD/CAM chain.
- If it is a conventional impression, it is cast in plaster by the dental technician, thus obtaining a replica of your tooth in the mouth.
- This plaster model is scanned by a 3D scanner, which allows to model your mouth in 3 dimensions.
- A specialised prosthetist (an info-prosthetist) will then virtually design your crown on the computer.
- Then a machine tool will machine a block of zirconia to make the cap.
- The screed is then placed in a furnace to obtain its final hardness (very close to that of metal).
All these steps are carried out in a laboratory in the Yvelines, by a team of experienced and qualified prosthetists.



What are the advantages of a zirconia crown?
- It allows to obtain an aesthetic result close to perfection, indeed its optical properties facilitate the task of the ceramist who does not need to hide the metal anymore. There can no longer be an unsightly black border between the crown and the gum, as there is no longer any metal.
- Zirconia is biocompatible and hypoallergenic. Furthermore, bacteria have great difficulty in adhering to zirconia, which is why gingival integration is excellent.
- The CAD/CAM manufacturing technique is much more precise than a metal casting. This precision of around 10 µm allows the crown to be adapted to the tooth in a way that is not possible with a metal framework crown. The crown is therefore better adapted, more watertight and therefore more durable over time. The risk of recurrence of caries under the crown is significantly reduced.
- Zirconia has exceptional physical and chemical properties that guarantee a long-lasting result.
- Since February 11, 2010, ceramic crowns (including the Zirconia crown) are registered in the NGAP (Nomenclature Générale des Actes Professionnels), and today in the CCAM (Classification Commune des Actes Médicaux), as such they are reimbursed like all other crowns by Social Security.




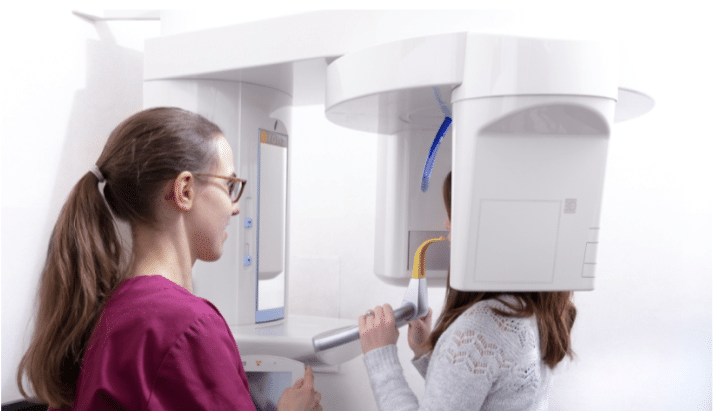
What is a Cone Beam?
First of all, the correct term is CBCT(Cone Beam Computerized Tomography).
It is in fact a kind of scanner, much less radiating thanks to the conical beam, and with a reduced field of view (8 cm x 8 cm in our practice). It is therefore specially dedicated to dental examinations.
What is a Cone Beam used for?
The Cone Beam is a fabulous diagnostic tool.
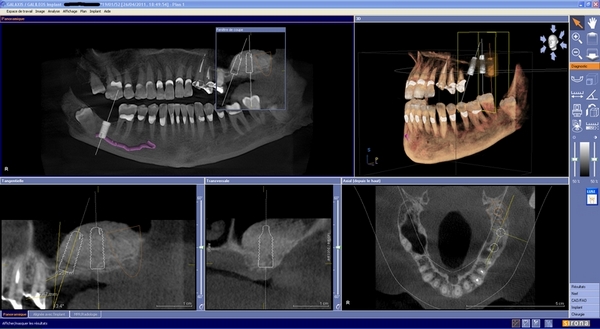
In a single image it is possible to radiograph the whole mouth, to reconstruct it virtually in 3 dimensions (3D) and to navigate in this space; millimetre by millimetre, cut by cut, visualising the teeth, the bone tissue, the main nerves, etc... and all this without deformation, without crushing the planes (unlike a panoramic) and with a formidable precision.
This tool therefore makes it possible to carry out screening (it is almost impossible to "miss" an infection with this type of examination), to refine a diagnosis, to explain a pathology, and thus to make therapeutic choices based on reality!
It is the examination of choice in implantology, as it allows us to visualise the available bone volumes and to protect noble structures such as nerves. We can now even merge the files from our optical camera with the images from the Cone Beam, for an even more accurate diagnosis. We can also export all these data to create a surgical guide on our machine! See a complete case here.
These 3D images can be studied in a software dedicated to implantology which allows to choose the size and the shape of the implants and to simulate their positions... virtually!
So you can see and understand your treatment!
Having such a tool in our dental practice has many advantages:
- All the steps are done in one place, so you don't have to go to a radiologist for this type of examination. This saves time for everyone.
- The result is instantaneous and allows the treatment plan to be validated immediately.
- When we perform complex procedures(Sinus Lift, Bone grafts, etc...) we can check the result immediately.
In a few months this tool has become indispensable to us.
Our profession as Dentists is constantly (r)evolving and the Cone Beam is a major advance.
Absolute contraindications
It is absolutely not possible to carry out these interventions in the following situations:
- HEART: heart diseases affecting the valves (valvulopathies), recent heart attack, severe heart failure, cardiomyopathies.
- MISCELLANEOUS: certain bone diseases, cancer in progress, certain immunological diseases, immuno-suppressive treatments, AIDS declared, organ transplants pending, certain psychiatric diseases, highly irradiated jawbones (radiotherapy treatment), treatment of osteoporosis or certain cancers with biphospnonates.
Complications (in case of oral surgery or implants) CAN BE SERIOUS.
For children, it is not possible to place an implant before the end of the growth of the jaws (usually 17-18 years).
Relative contraindications
These operations will be performed on a case by case basis, with caution in the following cases: insufficient bone, certain diseases of the mucous membrane of the mouth, periodontal disease (loosening), gums need to be cleaned and the disease stabilised beforehand, severe bruxism (patient clenching his teeth), unbalanced occlusal relationship (between the upper and lower teeth), infections of the neighbouring teeth (pockets, cysts, granulomas), severe sinusitis, poor hygiene of the mouth and teeth.

This list is by no means exhaustive and contraindications are left to the discretion of the practitioner who examined you.
Immediate complications
Anaesthetic risk, non-osteo-integration of the implant, infections, haemorrhages (not serious in most cases), nerve damage.
Late complications
Late failure - several years after placement - may be due to mechanical factors, loosening of the implant (as with a natural tooth), lack of hygiene or poor general condition.
Contra-indications bleaching
Bleaching is not recommended in many cases, especially for children's and teenagers' teeth, as well as for teeth with caries, wear or abrasion lesions, hypersensitivity (teeth that are very sensitive to cold), large or non-tight fillings.
Bleaching products, especially if used in high concentrations or repeatedly, have a demineralising effect on the hard tissues of the tooth and increase their permeability; in addition to the risk of mechanical embrittlement of the tooth, the dental pulp may be more exposed to chemical and thermal aggression. Finally, these products react with dental filling materials (amalgams, composites) and can damage the junction between the tooth and the filling, thus encouraging infiltration and recurrence of caries.
In view of these risks and contraindications, an examination of the teeth and the oral mucosa by the practitioner is essential before any tooth whitening treatment.
Source : http://www.sante.gouv.fr/quels-sont-les-risques-y-a-t-il-des-contre-indications.html
Contraindications veneers
Contraindications are parafunctions (bruxism), occlusal disturbances (too much malpositioning of the teeth), teeth that are too decayed, or periodontal problems (gum disease).
On the occasion of the Grand Angle programme on the Yvelines Première channel, Dr LUMBROSO was interviewed on the subject of "Taking care of your teeth".
Health: taking care of our teeth by Michaël Lumbroso
Interview with Dr Michaël LUMBROSO, Dental Surgeon in Versailles, broadcast on the local channel Yvelines Première on 12 April 2013.